DRIES BRAEKEN, Group Leader in the Life Science technologies department at imec, Leuven, Belgium
Neurodegenerative diseases such as Parkinson’s or Alzheimer’s are brain diseases hallmarked by the death of specific brain areas or progressive neuron loss. They have debilitating effects on movement, speech, and memory that are severe enough to impede everyday activities. Currently, there are more than one million people in Europe affected by Parkinson’s Disease (PD) and about seven million by a form of dementia. With an aging population, this number is expected to double in the next ten to twenty years, posing a major challenge to healthcare systems. So far, these brain diseases are incurable, and the neuron loss is irreversible. The search for effective treatments is difficult because we lack a fundamental understanding of disease mechanisms and causes and representative model systems to study them.
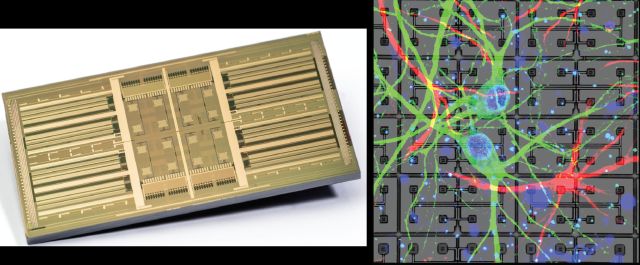
The rise of new chip technologies and genetic tools can help gaining insights in disease mechanisms and treatment strategies. Multi-electrode arrays (MEAs) have proven themselves as invaluable tools for this. MEAs are chips that can interrogate and interact with networks of neurons grown on top of them by either recording their electrical signatures or stimulating them (Figure 1). Imec’s high-density MEA packs thousands of electrodes in 1 mm2, thereby enabling an unprecedented resolution for neuronal interfacing. Combined with stem cell technology that can reprogram cells, the MEA can create and tweak any relevant brain circuit to study disease mechanisms and the effects of drugs on the circuits.

Parkinson’s disease
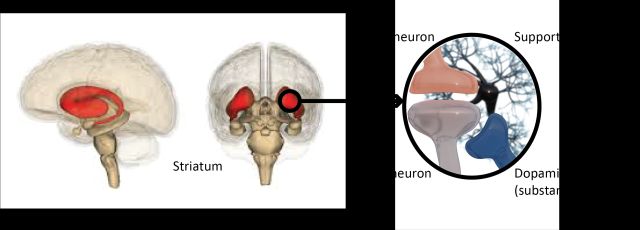
Parkinson’s disease (PD) is a neurodegenerative brain disorder that progressively affects movement and speech. The disease is related to the loss of dopamine-producing neurons in the substantia nigra. Neuronal death in this area causes miscommunication with connected brain structures responsible for movement (such as the striatum, shown in Fig. 2), resulting in the typical stumbling and shaking in these patients, but also depression, memory loss, and insomnia.

There is no cure for PD, but a number of treatments can alleviate symptoms. Almost all patients eventually need to take medication to help with their motor symptoms. When drugs are ineffective, more invasive options such as deep brain stimulation surgery can be considered. The treatment is highly individualized and adjusted over time based on symptoms and side effects.
Key problems in PD
What makes it so difficult to find a cure for this disease? In short, it is the lack of relevant model systems that recapitulate all the disease features observed in patients. First, we do not have direct access to diseased tissue. Human brains are only available post-mortem, and at that time, the brain areas most interesting for PD research have died. Secondly, patients are currently diagnosed based mostly on motor symptoms, but the dopaminergic neurons are already damaged or gone by the time these symptoms appear. We need to study the brain regions before the damage occurs to understand disease onset and progression.
The third challenge is the lack of human-specific aspects in the current model systems. Animal models have played a vital role in preclinical research for drug discovery. However, over the last 20 to 30 years, they haven’t led to any new drugs for Parkinson’s. Chemical models mimic the dopaminergic loss and associated motor effects but cannot be used to study disease progression or mechanisms. Genetic models, on the other hand, offer the possibility of investigating disease pathology but only display a mild to no phenotype at all. In vitro cell-based models have focused on induced pluripotent stem cells (iPSCs) from patients and reprogramming them into brain cells. However, these are not embedded in a neural circuit, while motor problems arise from network dysfunction.
How to make a brain with PD
To overcome the obstacle of finding suitable tissue to study and experiment on, our team proposes to build a human brain-on-chip model. This unique strategy’s cornerstones are the iPSCs (Induced pluripotent stem cells) technology combined with an army of transcription factors and imec’s high-density CMOS-MEA (multi-electrode array) with individually addressable electrodes. Together, they make it possible to recreate any relevant brain circuit in the lab, on a chip.
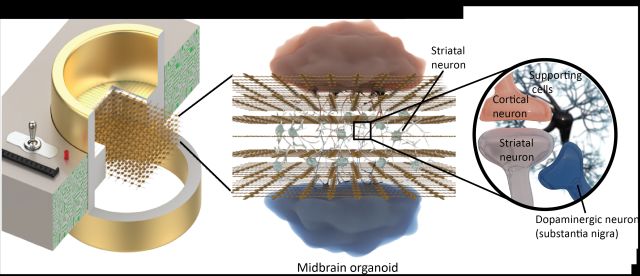
How does it work for PD? Many of the substantia nigra’s effects are mediated through the striatum. This brain area receives input from the dopaminergic neurons (in the substantia nigra) and cortical neurons. An imbalance in this circuit causes motor problems and other PD-related symptoms. That’s why researchers are now building this circuit from patient-specific cells (Figure 3).


Programming cells on a MEA
In a first step fibroblast progenitor cells are harvested from a patient’s skin and plated on the MEA. The imec MEA consists of 16.384 individually steerable electrodes at single-cell resolution. The electrodes are spaced so close together (15 µm pitch) that each cell is in contact with at least one electrode. By sending a small current through the electrode, tiny transient holes can be made in the cell in a process called electroporation. Transcription factors are then applied on the cells and enter through the holes to reprogram the cell into brain cells.
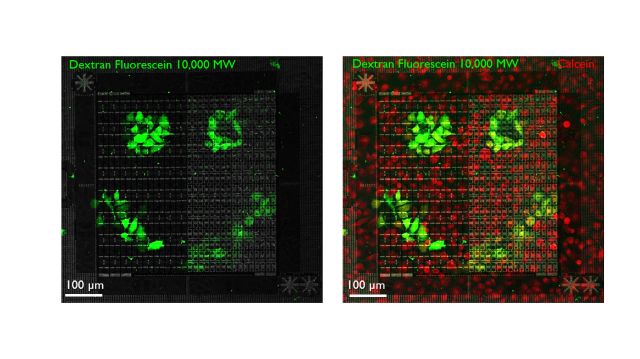
Because the MEA can access single cells, researchers can build the striatal circuit by choosing which cells are becoming either cortical, striatal, or dopaminergic (nigral) cells on specific locations of the chip (Figure 4). By selectively activating the electrodes, a variety of patterns can be built to create microcircuits. The MEA fits into a cell culture incubator and connects to a computer with a custom user interface. The idea is that the system will be distributed over different labs to initiate a global partnership.

Unique chip signatures
The hypothesis of the researchers is that these brain microcircuits have unique signatures. Ten percent of PD patients have a clear genetic mutation while 90% (‘sporadic’ patients) probably have a complex gene pattern involvement that is yet unknown. In a first approach, the researchers will plate cells from people with a known mutation on the MEA to characterize their electrophysiological phenotype (parameters such as neuron firing rate, signal propagation, or burst patterns) and compare them to cells from healthy individuals. Once differentiating features have been established and categorized, the brain cells of the sporadic patients can be studied, and their phenotypes can be subdivided into one of the categories in a process called stratification (Figure 5).

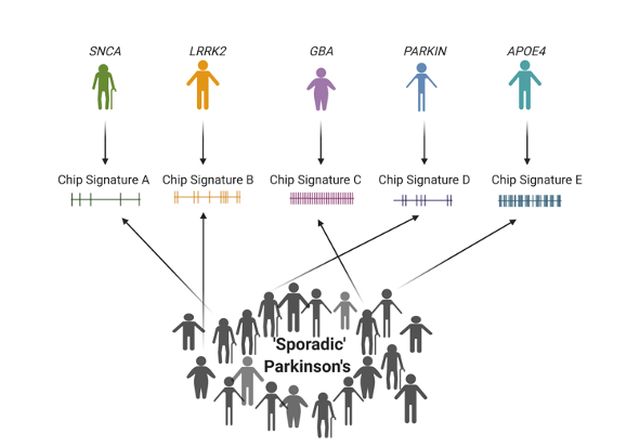
Figure 5. Sporadic PD patients can be classified via their electrophysiological profile in a process called stratification.
The implications of this strategy are enormous. It enables PD to be objectively defined by solid quantifiable phenotypes, rather than by the typical movement symptoms currently used to examine and diagnose the disease. In turn, this approach could lead to targeted therapies to slow down or completely halt the disease. There are indeed already therapies available to intervene in certain processes. The problem for pharmaceutical companies is that only ten percent of hereditary PD patients and that this small group is spread out worldwide. As an alternative, Mission Lucidity will offer the possibility of performing drug studies on the entire patient population that are divided into groups based on their molecular and electrophysiological profile.
The brain is 3D…
Once we know what the circuit looks like in a PD patient, we can manipulate it and study the effect of these manipulations, for example, by introducing changes in the genes and pathways using genetic tools such as CRISPR-Cas9, or by applying drugs. We can also add more cells, effectively making the circuit more complex and thus better representing the patient’s actual brain circuit: aside from the three neuron types that are currently studied, it would also be interesting to look at the effects on inflammatory cells such as microglia and astrocytes. This could be conceived as a test for the strength and validity of the circuit model.
The brain is, of course, more than a two-dimensional layer of cells. It is a 3D organ where neurons receive inputs from multiple angles, which is likely relevant for neuronal computation and information processing. In the next few years, Dries’ team at imec aims to implement 3D structures in their research. Besides the traditional 2D models, more complex 3D cultures and organoids (in vitro organs) are being developed worldwide. Organoids are increasingly improving from disorganized cellular blobs to structured organs containing circuits.
…and so will be the MEA
Using this kind of 3D structure has implications for the MEA, which is still 2D. Imec is working on a 3D MEA by stacking several MEAs on top of each other. Moreover, they will remove most of the silicon, forming a mesh with holes and nodes. That way, the cells in the organoids can grow through the openings, establishing contact with the electrodes in three dimensions (Figure 6). The goal is to maintain the resolution that the 2D MEA already offers even though mm-size organoids contain far more cells to record from. It is a challenge that researchers already faced in the development of neuroprobes. Now, with the high-density Neuropixels brain implant, we can record signals from many cells in a specific brain volume. The difference is that when implanting a neuroprobe, the ‘pre-existing brain’ is the limit, and moving to another brain area in a circuit often requires a second device. With the MEA, we can build our own circuits around the electrodes.

In the next decade, the goal is –aside from moving to 3D– to use the technology as a screening tool to tackle other diseases. Currently, circuits are built on a single chip. With high-throughput screening devices, we have access to a large amount of patient data on which AI systems can detect patterns. Furthermore, the technology to create 2D and later 3D brain-on-chip models can also be used to reconstruct neural networks in other neurodegenerative diseases, including Amyotrophic Lateral Sclerosis (ALS) and Alzheimer’s. The new tools will enable the stratification of patients and the testing of new, personalized therapeutic approaches.
Mission Lucidity
Mission Lucidity brings clinicians, scientists, and engineers from imec, KU Leuven, UZ Leuven, and VIB together to gain a deeper understanding of neurodegenerative disorders with the ultimate goal of curing and preventing them. It combines the expertise of best-in-class partners in nanotechnology, biomedical research, and clinical care –precisely the kind of unique interdisciplinary ecosystem that is required for delivering scientific and medical breakthroughs in this field. In Fall 2018, the efforts of the team were recognized in receiving the prestigious Collaborative Science Award from the Chan Zuckerberg Initiative (CZI) for the brain-on-chip project and an invitation to join the Neurodegeneration Challenge Network.
Brain-on-chip, the project focused on beating Parkinson’s disease described in this article, is currently the most advanced. However, Mission Lucidity has projects in the pipeline that focus on other neurodegenerative diseases and technologies:
– TRIAGE: For this project, researchers are developing a chip as a screening tool to assess individual risk profiles for Alzheimer’s disease (AD). This research will help identify people who are at risk and define patient subgroups that are likely to benefit from specifically tailored treatments. The project is still in the first phase in which the link between risk genes, immunology, and AD is being investigated. Technological developments involving imec’s MEA will follow in a future phase.
– ADMIRE: Here, researchers will use an advanced hyperspectral camera to scan the retina, the most accessible part of our brain, for early signs of AD even before the first symptoms appear. A faster diagnosis tool will enable studying disease progression, providing individualized patient care, and evaluate the success of new therapies. Imec’s hyperspectral cameras have already been successfully applied to microscopes and retinal fundus cameras for this application. The first results were recently accepted for publication in the Journal of Alzheimer’s Research & Therapy.
– TESCoGEN: Using minimally invasive epicranial stimulation, the goal of this project is to preserve neurons in brain regions that are involved in cognitive functioning. This project is still in the proposal phase.
About the author
Dries Braeken received a MSc degree in Biomedical Sciences from KU Leuven, Belgium, in 2003, and a Ph.D. degree in Medical Sciences from the KU Leuven (in collaboration with imec, Leuven, Belgium) in 2009. He has been a Group Leader in the Life Science technologies department at imec since 2017. He is (co)-author of more than 80 internationally peer-reviewed publications and 13 granted and pending patents. His research interests are developing and validating silicon technologies for cell and tissue interfacing in healthcare applications.